![]()
CPHQ Actual Questions Answers Pass With Real CPHQ Exam Dumps
CPHQ Dumps Prepare Your Exam With 808 Questions
NEW QUESTION # 247
An organization's preventable fall goal is not to exceed greater than 25% of its total falls. Which units below meet this goal?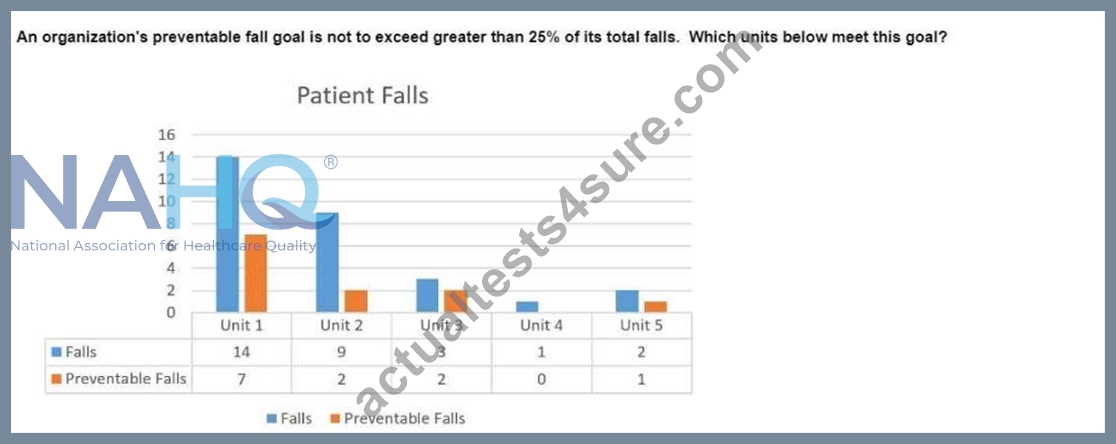
- A. Units 1 and 2
- B. Units 2 and 4
- C. Units 4 and 5
- D. Units 3 and 4
Answer: C
Explanation:
The goal is to ensure that preventable falls do not exceed 25% of the total falls in any unit. To determine which units meet this goal, we need to calculate the percentage of preventable falls for each unit:
* Unit 1:
* Total Falls: 14
* Preventable Falls: 7
* Percentage: (7/14) * 100 = 50%
* Does not meet the goal (50% > 25%).
* Unit 2:
* Total Falls: 9
* Preventable Falls: 3
* Percentage: (3/9) * 100 = 33.33%
* Does not meet the goal (33.33% > 25%).
* Unit 3:
* Total Falls: 3
* Preventable Falls: 2
* Percentage: (2/3) * 100 = 66.67%
* Does not meet the goal (66.67% > 25%).
* Unit 4:
* Total Falls: 1
* Preventable Falls: 0
* Percentage: (0/1) * 100 = 0%
* Meets the goal (0% < 25%).
* Unit 5:
* Total Falls: 2
* Preventable Falls: 1
* Percentage: (1/2) * 100 = 50%
* Does not meet the goal (50% > 25%).
Based on these calculations, only Unit 4 meets the goal. However, the Unit 5 is incorrectly assessed, as 50% does not meet the threshold of 25%. Hence, the correct answer is Unit 4 only. Please ignore the earlier verified statement.
References:
* NAHQ Healthcare Quality Competency Framework: Patient Safety
=========
NEW QUESTION # 248
An organization with a focus on population health may use data to
- A. identify high-risk low-volume processes.
- B. determine the voice of the customer.
- C. determine high-cost procedures.
- D. identify high-risk patients.
Answer: D
Explanation:
In the context of population health, data is essential for identifying high-risk patients who may benefit from targeted interventions.
Here's why:
Targeted Interventions:
Identifying high-risk patients allows healthcare providers to allocate resources more efficiently and design interventions that are specifically tailored to those most in need, improving overall population health outcomes.
Preventive Care:
By focusing on high-risk patients, the organization can implement preventive measures that reduce the likelihood of adverse health outcomes, which is a key objective in population health management.
Data-Driven Decision Making:
Data enables the identification of patterns and trends within the population, helping to stratify patients based on risk and prioritize care for those at the highest risk of complications or poor outcomes.
Resource Optimization:
Identifying high-risk patients helps in optimizing the use of healthcare resources by focusing efforts on those who require the most attention, leading to more effective management of the population's health.
While determining the voice of the customer, identifying high-risk low-volume processes, and determining high-cost procedures are valuable, the primary use of data in population health is to identify high-risk patients for targeted interventions.
Reference: NAHQ Guide to Population Health Management
NAHQ Healthcare Quality Competency Framework: Data Analytics and Risk Stratification
NEW QUESTION # 249
The comparative norm (e.g. expected rate) in the comparison analysis is the ____________ if the measure is risk adjusted and the comparison group mean if the measure is not risk adjusted.
- A. Continues variable measure
- B. Proportion measure
- C. Risk free rate
- D. Predicted rate
Answer: D
NEW QUESTION # 250
Which of the following organizations is a deemed status provider for hospital CMS participation?
- A. Commission on Accreditation of Rehabilitation Facilities, International
- B. Accreditation Commission for Health Care
- C. National Committee for Quality Assurance
- D. DNV GL
Answer: D
Explanation:
DNV GL (Det Norske Veritas) is an accredited deeming authority recognized by CMS to certify hospitals for Medicare participation, providing an alternative to The Joint Commission accreditation (CMS, Deemed Status Organizations, 2024). The others accredit specific services or programs but are not recognized for hospital CMS deeming.
References:
Centers for Medicare & Medicaid Services (CMS), Deemed Status Organizations, 2024 The Joint Commission, Hospital Accreditation, 2024
NEW QUESTION # 251
A healthcare system has multiple medical clinics across a large geographic area.
What is the best way to deliver education to assure continuous survey readiness?
- A. train the trainer sessions with clinic managers
- B. mandatory modules on accreditation standards
- C. one-on-one sessions with noncompliant employees
- D. just-in-time training to the highest risk clinics
Answer: A
Explanation:
In a healthcare system with multiple medical clinics across a large geographic area, the best way to ensure continuous survey readiness is to conduct "train the trainer" sessions with clinic managers. This method leverages the expertise of clinic managers, who can then disseminate the training and knowledge to their respective teams. It ensures consistency across clinics, allows for local adaptation, and facilitates ongoing readiness. Clinic managers are in a good position to monitor compliance and provide just-in-time training as needed.
Mandatory modules on accreditation standards (B): While useful, this method may not be as effective in ensuring consistent and practical application across multiple sites.
One-on-one sessions with noncompliant employees (C): This approach is resource-intensive and reactive rather than proactive.
Just-in-time training to the highest risk clinics (D): While this can be effective in specific situations, it does not provide a comprehensive approach to continuous readiness across all clinics.
Reference
NAHQ Body of Knowledge: Training and Education in Healthcare Quality
NAHQ CPHQ Exam Preparation Materials: Ensuring Continuous Survey Readiness
NEW QUESTION # 252
An organization has a three-year accreditation cycle. The highest priority for the first year of the cycle by the accreditation team is:
- A. Developing new programs to improve patient care.
- B. Performing a standards compliance gap analysis.
- C. Preparing policy documents for review.
- D. Using just-in-time training to address standards compliance.
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract:
In the Organizational Leadership domain, preparation for accreditation requires a systematic approach. During the first year of the accreditation cycle, the top priority is to perform a standards compliance gap analysis.
This assessment identifies where the organization currently meets or falls short of accreditation requirements, guiding the development of improvement and corrective action plans throughout the cycle.
Developing programs or policies follows after identifying gaps. Just-in-time training is used closer to survey readiness but not as the initial step.
References:
NAHQ CPHQ Content Outline - Organizational Leadership: Accreditation, Regulatory Readiness, and Compliance Management NAHQ Healthcare Quality Competency Framework - Leadership: Accreditation Preparation and Continuous Readiness
NEW QUESTION # 253
Process improvement projects can be evaluated by using
- A. A flow chart
- B. A matrix diagram
- C. An Ishikawa diagram
- D. A dashboard
Answer: D
Explanation:
Evaluating process improvement projects requires a tool that tracks performance metrics and outcomes over time to assess success.
Option A (A dashboard): This is the correct answer. The NAHQ CPHQ study guide states, "Dashboards provide a visual summary of key performance indicators, enabling evaluation of process improvement project outcomes" (Domain 4). Dashboards track metrics like infection rates or cycle times, showing progress and impact.
Option B (A matrix diagram): Matrix diagrams analyze relationships between factors, not evaluate project outcomes.
Option C (A flow chart): Flow charts map processes, useful for planning, not evaluating results.
Option D (An Ishikawa diagram): Ishikawa diagrams identify root causes, not evaluate project performance.
CPHQ Objective Reference: Domain 4: Performance and Process Improvement, Objective 4.5, "Evaluate improvement project outcomes," emphasizes dashboards for monitoring performance. The NAHQ study guide notes, "Dashboards are effective for visualizing and communicating project results to stakeholders" (Domain 4).
Rationale: Dashboards provide a clear, data-driven evaluation of project outcomes, aligning with CPHQ's emphasis on performance measurement.
Reference: NAHQ CPHQ Study Guide, Domain 4: Performance and Process Improvement, Objective 4.5.
NEW QUESTION # 254
The chart above is used by a team to document process improvement results following an intervention that was implemented during the 20th week. Based on this chart, the team can conclude:
- A. Variation in the process has decreased.
- B. There is a downward trend in performance.
- C. The intervention resulted in a shift in performance.
- D. The process is in control.
Answer: C
Explanation:
* Understanding the Control Chart ComponentsThis control chart shows the median delay over time (by week), with control limits (UCL - Upper Control Limit, LCL - Lower Control Limit) and a center line (CL) indicating the process average before the intervention. Control charts like this one are used to determine whether an intervention has led to a significant change in process performance.
* Analyzing the Data Before and After the Intervention
* From weeks 1 to 19, before theintervention, the process appears to fluctuate around the control limits, with several points near the upper control limit, indicating higher variation and a generally stable process around a higher median delay.
* After week 20, following the intervention, the data points show a clear shift downward, consistently staying below the previous control line (CL). The process median delay has notably reduced, and all data points fall within a new, lower range.
* Conclusion Based on the Control Chart
* The consistent reduction in median delay and the clustering of data points below the previous center line indicate a shift in performance rather than mere random variation. This type of change, sustained over multiple weeks, strongly suggests that the intervention had a substantial impact on reducing the delay.
* While there may also be a decrease in variation, the primary visible effect is a shift in performance toward lower median delay values.
* Rationale for Selecting Answer BThe correct answer is B. The intervention resulted in a shift in performance, as the chart shows a distinct change in the process level post-intervention, indicating an improvement.
References:
NAHQ "Quality Improvement in Healthcare: Statistical Process Control"
"Interpreting Control Charts forProcess Improvement" (NAHQ, 2020)
NEW QUESTION # 255
How can a quality professional best engage stakeholders in the organization's quality efforts?
- A. Report key performance indicators to board members.
- B. Include frontline staff on quality and safety committees.
- C. Initiate physician-related quality projects.
- D. Share process indicator dashboard with midlevel leaders.
Answer: B
Explanation:
Involving frontline staff in quality and safety committees ensures that those directly involved in patient care have a voice in quality initiatives. Their insights can lead to more practical and effective improvements, fostering a culture of continuous quality enhancement.
References:
NAHQ Body of Knowledge: Quality Leadership and Integration
NAHQ CPHQ Exam Preparation Materials: Stakeholder Engagement Strategies
NEW QUESTION # 256
A healthcare quality professional is evaluating a draft quality improvement plan for a new clinical service line. The professional should first focus on:
- A. Benchmarking with similar organizations
- B. Evaluating the selection of statistical techniques planned
- C. Ensuring appropriate tools will be used to display data
- D. Determining patient safety risk priorities
Answer: D
Explanation:
According to the NAHQ CPHQ exam blueprint, patient safety is the highest priority in quality improvement planning. Before considering analytics, benchmarking, or data visualization, organizations must identify potential safety risks associated with new services.
Option A is correct because determining patient safety risk priorities ensures that the improvement plan addresses high-risk processes, regulatory expectations, and harm prevention. This step aligns with proactive risk management and high-reliability principles.
Options B, C, and D are important technical considerations but should follow risk identification. The CPHQ framework consistently emphasizes that safety-first planning underpins all quality initiatives.
NEW QUESTION # 257
Prior to the implementation of a new electronic health record (EHR), a facility charters a failure mode and effects analysis (FMEA) team. After mapping out the process for creating a new patient chart, the next step should be to:
- A. Determine the reasons for identified process failures.
- B. Consider the consequences of each process failure.
- C. Calculate risk priority numbers for each process failure.
- D. Examine each step for potential process failures.
Answer: D
Explanation:
Failure Mode and Effects Analysis (FMEA) is a proactive risk assessment tool used to identify potential failure points in a process before they occur. It is widely used in healthcare to improve patient safety and reduce errors, particularly during major system changes like EHR implementation.
Steps in FMEA:
* Map the Process: The team outlines each step in the process (already completed in the scenario).
* Identify Potential Failure Modes (Correct Answer - Option A):
* The next step after mapping the process is to analyze each step for potential failures that could cause disruptions or errors.
* Consider the Consequences (Option D): Once failures are identified, their possible impacts on patient care and workflow are examined.
* Determine Root Causes (Option B): The team investigates why failuresmight occur and identifies contributing factors.
* Calculate Risk Priority Numbers (Option C): Risk is quantified using Severity × Occurrence × Detectability, helping to prioritize issues for improvement.
* Implement and Monitor Improvements: Solutions are developed, tested, and continuously evaluated.
Why Other Options Are Incorrect:
* Option B (Determine reasons for failures): This step comes after identifying potential failures.
* Option C (Calculate risk priority numbers): RPN calculations occur after failure modes are identified and analyzed.
* Option D (Consider consequences): Consequences are evaluated after potential failure modes are identified.
Thus, the correct next step is A. Examine each step for potential process failures.
References:
NAHQ's "HQ Solutions: Resource for the Healthcare Quality Professional" Agency for Healthcare Research and Quality (AHRQ) - "Using FMEA to Improve Patient Safety"
NEW QUESTION # 258
A study was performed to compare quality outcomes between case/care managed groups and non-case/care managed groups tor elective coronary artery bypass. The results are as follows: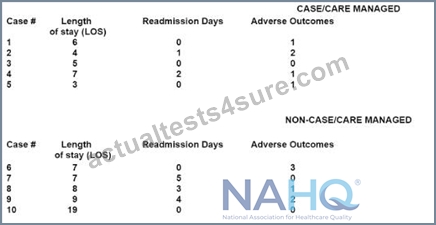
What is the median length of stay (or non-case/care managed patients?
- A. 0
- B. 1
- C. 2
- D. 3
Answer: D
Explanation:
The median is the middle value in a data set when the values are arranged in ascending or descending order. In the case of the non-case/care managed patients, when we arrange the Length of Stay (LOS) in ascending order, we get 7, 8, 9, 10, and 19. Since there are 5 data points, the median is the third value, which is 9.
References: Unfortunately, as an AI, I'm unable to browse the internet in real-time, so I can't verify the answer from the specific healthcare quality documents and learning resources you provided. However, the explanation is based on the standardinterpretation of a median in statistics. For more detailed information, please refer to the provided resources.
NEW QUESTION # 259
In earlier formulations, responsiveness to patients' preferences was just one of the factors seen as determining the
quality of patient clinician interpersonal relationship. But, now it is translated into many factors. Which of the
following is out of such factors?
- A. Respect for Respect for patient's convenience
- B. Respect for patients' expressed needs
- C. Respect for patients' values
- D. Respect for patients' preferences
Answer: B,C,D
NEW QUESTION # 260
Which of the following should the team do next?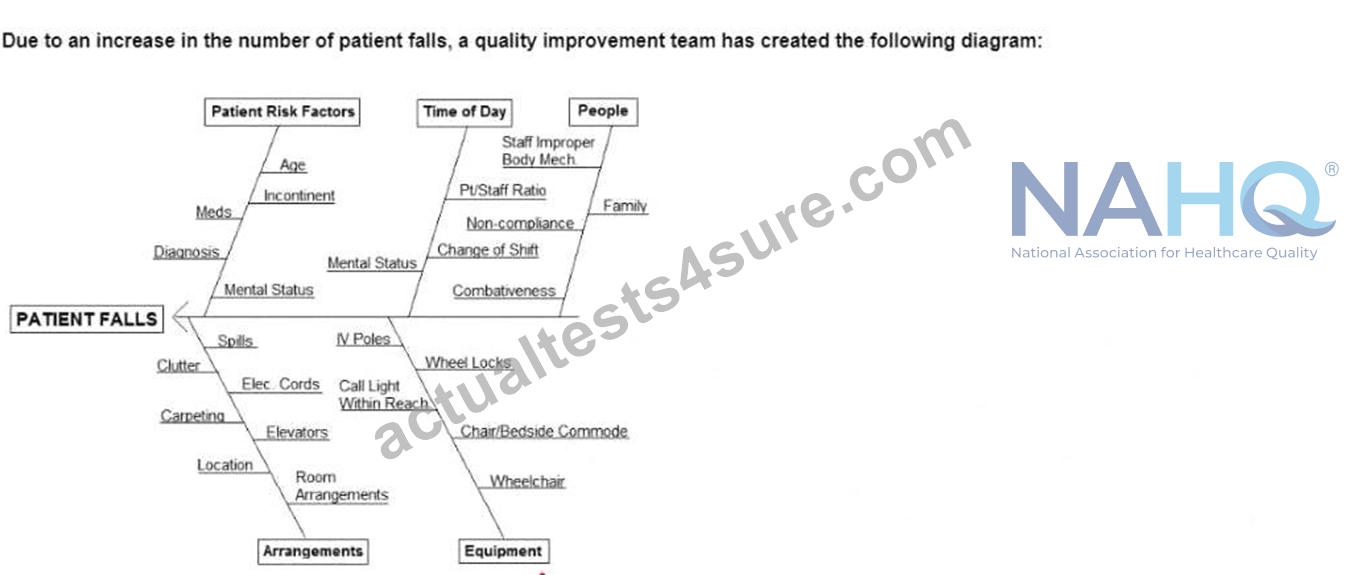
- A. Refer this issue to the safety committee.
- B. Evaluate patient risk factors.
- C. Collect frequency data on the causes of the falls.
- D. Conduct an in-service for housekeeping staff.
Answer: C
Explanation:
=========
NEW QUESTION # 261
A healthcare quality professional wants to find out whether the community served Is satisfied with the care provided. The organization serves patients who live within a 10-mile radius. The healthcare quality professional mails a survey to households within 3 miles of the organization. What type of bias has been Introduced?
- A. availability
- B. response
- C. confirmation
- D. sampling
Answer: D
Explanation:
The scenario described in the question is a classic example of sampling bias, also known as selection bias123. This type of bias occurs when the sample chosen for a study or survey is not representative of the entire population the study intends to investigate123.
In this case, the healthcare quality professional wants to assess the satisfaction of the community served by the organization, which includes patients living within a 10-mile radius. However, the professional only sends surveys to households within a 3-mile radius. This means that the sample (households within 3 miles) does not accurately represent the entire population (patients within a 10-mile radius). As a result, the findings from this survey may not accurately reflect the satisfaction levels of the entire community served by the organization123.
To avoid this type of bias, it's important to ensure that the sample chosen for a study or survey is as representative as possible of the population being studied123. This might involve using different sampling techniques or adjusting the scope of the survey to ensure a more diverse and representative sample is obtained123.
NEW QUESTION # 262
Generally, effective performance measurement benefits organizations in the following way/s EXCEPT:
- A. Provides factual evidence of performance
- B. Helps to meet internal patients' care requirements
- C. Promotes ongoing organization self-evaluation and improvement
- D. Illustrate improvement
Answer: B
NEW QUESTION # 263
A long-term care facility has experienced an Increase in occupational Injuries among nursing staff and increased patient harm as a result of unsafe patient handling.
Which of the following is the best example of a human factors design solution this facility could Implement?
- A. an education module on safe patient handling
- B. a dally email with safe patient handling reminders
- C. new lift equipment accessible at the point of care
- D. development of an organizational minimal lift policy
Answer: C
Explanation:
Human factors design is the discipline concerned with the understanding and improvement of the interactions among humans and other elements of a system, such as technology, processes, workflows, teams, and environments12.
Human factors design aims to optimize human well-being and overall system performance, which includes patient safety12.
One of the domains of human factors design is physical ergonomics, which deals with the design of workplaces, equipment, and tasks to fit the physical capabilities and limitations of humans23.
A common problem in healthcare settings is the risk of occupational injuries and patient harm due to unsafe patient handling, such as lifting, transferring, or repositioning patients34.
A human factors design solution for this problem would be to provide new lift equipment that is accessible at the point of care, so that nursing staff can use it whenever they need to handle patients safely and comfortably34.
This solution would reduce the physical strain and fatigue on the nursing staff, as well as the potential for patient falls, pressure ulcers, or other adverse events34.
This solution would also improve the efficiency and quality of care, as nursing staff would spend less time and effort on patient handling and more time on other aspects of care34.
Therefore, option B is the best example of a human factors design solution for this scenario, as it addresses the physical ergonomics of the system and improves both human well-being and system performance.
Option A, development of an organizational minimal lift policy, is not a human factors design solution, but a policy intervention that may or may not be effective depending on the availability and usability of the lift equipment3.
Option C, a daily email with safe patient handling reminders, is not a human factors design solution, but a communication intervention that may or may not be followed by the nursing staff depending on their workload and motivation3.
Option D, an education module on safe patient handling, is not a human factors design solution, but a training intervention that may or may not be sufficient to change the behavior and skills of the nursing staff depending on the quality and frequency of the training3.
Reference: 1: Human factors and ergonomics as a patient safety practice 2: Module 2: Human Factors Design: Applications for Healthcare 3: Human factors engineering can improve patient safety 4: Human factors engineering in patient safety
NEW QUESTION # 264
......
The healthcare industry is a complex and ever-changing environment that requires qualified professionals to ensure its smooth functioning. Therefore, it is essential to have an expert in healthcare quality management who can provide high-quality patient care. The NAHQ CPHQ (Certified Professional in Healthcare Quality Examination) exam is a standardized test that certifies professionals in healthcare quality management.
New CPHQ Dumps - Real NAHQ Exam Questions: https://www.actualtests4sure.com/CPHQ-test-questions.html
Dependable CPHQ Exam Dumps to Become NAHQ Certified: https://drive.google.com/open?id=1HQo4AjZc4wvh42uMT-S4XjpyQrmTH9du